IT began with a bird-watching excursion on the remote island of Saint Helena – and it ended, for three people, in death. For the rest of the world, the outbreak of the Andes hantavirus strain aboard the Dutch-flagged expedition cruise ship MV Hondius has become the most alarming new pathogen event of 2026: a rare, rodent-borne killer that has, for the first time in recorded history, gone genuinely international.
Now, as fear ripples outward from the South Atlantic to the shores of southern Africa and beyond, Zimbabwe and South Africa have stepped into the breach – not with alarm, but with the measured, science-anchored language of governments that understand what is at stake when rumour outruns response.
The story of the MV Hondius outbreak is, at its core, a story about the globalisation of risk. The vessel departed Ushuaia, Argentina, on 1 April 2026 – deep inside Andes virus territory – carrying 147 passengers and crew from 23 countries on an expedition through ecologically extreme environments: mainland Antarctica, South Georgia, Nightingale Island, Tristan da Cunha, Saint Helena, and Ascension Island.
Somewhere along that route – most likely during shore excursions on islands home to infected rodent populations – exposure occurred. The index case, a 70-year-old Dutch national, died on board on 11 April 2026. His widow disembarked at Saint Helena showing symptoms, deteriorated mid-flight to Johannesburg, and died upon arrival at a Kempton Park hospital on 26 April. She was the virus’s first African fatality. A third passenger, a German national, died aboard the ship on 2 May. A critically ill British passenger was medically evacuated from Ascension Island to a Sandton ICU, where South Africa’s National Institute for Communicable Diseases (NICD) would make the identification that changed everything.
By the time the WHO received formal notification on 2 May 2026 – a full 21 days after the index case’s death – the virus had touched multiple continents: its probable origin in South America, its first fatalities in the South Atlantic and southern Africa, its subsequent spread among European nationals repatriated from Tenerife to the Netherlands, Germany, France, Spain, and Switzerland. A suspected case on the tiny island of Tristan da Cunha – a community of 220 people with no airstrip – required the extraordinary deployment of British military paratroopers, who parachuted in from an RAF A400M Atlas to deliver 3,300 kilograms of medical supplies.
As of 11 May 2026, the WHO had confirmed seven cases of hantavirus infection with two additional probable cases awaiting laboratory results, and a death toll of three. The US Centers for Disease Control and Prevention has classified the response as a ‘Level 3’ emergency. The case fatality rate in this cluster – approximately 43 percent – is chilling, already exceeding the Andes virus’s historically terrifying average of 30 to 50 percent.

OUTBREAK AT A GLANCE — MV HONDIUS HANTAVIRUS CLUSTER
| INDICATOR | STATUS AS OF 12 MAY 2026 |
| Confirmed cases | 7 confirmed; 2 additional probable cases pending |
| Deaths | 3 (Dutch national aboard; Dutch national in Johannesburg; German national aboard) |
| Critical cases | 1 British national in ICU, Sandton, South Africa |
| Countries affected | 13+ — Netherlands, Germany, Spain, France, Switzerland, UK, South Africa, Cape Verde, Canada and others |
| Virus strain | Andes virus (ANDV) — the ONLY known hantavirus capable of human-to-human transmission |
| WHO global risk assessment | LOW — limited human-to-human spread; outbreak traced to expedition contacts |
| Africa’s exposure | 2 confirmed deaths in South Africa; 3 Zimbabwean healthcare workers returned as asymptomatic contacts |
| Treatment/Vaccine available? | NO — no licensed antiviral or vaccine exists; treatment is intensive supportive care only |
ZIMBABWE’S RESPONSE
Harare Acts: Three Returned Workers, a 45-Day Watch, and a Government Holding the Line
Zimbabwe’s direct exposure to this crisis arrived not in the form of confirmed patients, but in the form of possibility, which is, in many ways, the more difficult thing to manage. Three Zimbabwean healthcare workers, deployed to Ascension Island, were identified as contacts of a confirmed hantavirus case during their time on the British Overseas Territory. They were repatriated on Monday, 12 May 2026.
The critical early fact: all three tested negative in PCR tests conducted on Sunday, 11 May, and were confirmed healthy and asymptomatic on arrival. Yet Zimbabwe’s Ministry of Health and Child Care (MoHCC) has adopted the precautionary posture of a government that understands the difference between ‘not positive yet’ and ‘safe.’
Health Minister Douglas Mombeshora told a press briefing in Harare that the three individuals will undergo active monitoring for a period of 45 days – the full outer bound of the Andes virus incubation window, which WHO guidance places at between 4 and 42 days from exposure. Port Health Services conducted initial screening and assessment at Robert Gabriel Mugabe International Airport on arrival. The workers will be housed together in a designated private isolation facility for the quarantine period, with appropriate infection prevention and control measures in place throughout.
“There is no indication that the travelers pose a public health risk,” Mombeshora said — a formulation precise enough to be honest about present evidence, without making promises science cannot keep about the weeks ahead.
The protocol Zimbabwe has adopted is, in structural terms, textbook: screen on arrival; activate the full incubation-window monitoring period; isolate as a cohort in a controlled environment; implement infection control throughout. Its significance lies less in novelty than in execution — in whether a health system battered by decades of under-resourcing can deliver on the rigour those words require for 45 unbroken days.
ZIMBABWE’S DECLARED PRECAUTIONARY MEASURES — MOHCC PROTOCOL
| # | MEASURE |
| 1 | Screening and assessment by Port Health Services upon arrival at Robert Gabriel Mugabe International Airport. |
| 2 | Active monitoring for hantavirus symptoms during the full recommended 45-day observation period — aligned with the outer limit of Andes virus incubation, as advised by WHO. |
| 3 | All three travellers are to remain together in a designated private isolation facility for the duration of the quarantine period. |
| 4 | All three travellers to remain together in a designated private isolation facility for the duration of the quarantine period. |
SOUTH AFRICA’S ROLE
The Patient in Sandton, the Scientists Who Found the Virus, and a Country That Held Its Nerve
South Africa has been the most consequential African actor in this outbreak — and its role is twofold: as a country that received, treated, and in one case failed to save patients from the stricken ship, and as the continent’s forensic anchor, the nation whose scientists identified what the world was dealing with.
On 1 May 2026, a public holiday, an email arrived at the inbox of Professor Lucille Blumberg of the NICD from a concerned colleague in the United Kingdom: a British infectious disease specialist who sensed something was badly wrong aboard the MV Hondius. Within 24 hours, Blumberg’s team had confirmed hantavirus in the critically ill British patient in the Sandton ICU. By 6 May, viral sequencing identified the specific strain as Andes virus — a result of extraordinary significance, since Andes is the only one of the 38 known hantavirus variants documented to spread between humans.
“It is not a virus we see in this country,” Blumberg told Parliament’s Portfolio Committee on Health this week. “And it is not the usual cause of respiratory infection outbreaks on ships.” In normal circumstances, investigators would have looked first at Legionella or influenza. Instead, the NICD team drove through every possibility on an extensive respiratory pathogen panel – and found the needle in a very unusual haystack.
The parallel story is grimmer. A 69-year-old Dutch woman – the widow of the index case – collapsed on flight KL592 to Johannesburg on 25 April and died at the OR Tambo International Airport emergency department on 26 April. She had spent 45 minutes aboard the plane in acute distress. Contact tracing for her fellow passengers was immediately initiated. The NICD later confirmed her PCR-positive for Andes hantavirus. Her remains were repatriated to the Netherlands on Thursday.
The British patient evacuated from Ascension Island on 27 April remains hospitalised in the Sandton ICU – critically ill but stable, the outlier who survived the virus’s most brutal phase, and who stands as both a medical challenge and a symbol of what intensive care, deployed swiftly, can do against a pathogen for which no antiviral exists.
South Africa’s health authorities have since drawn commendation from across the political spectrum. The Portfolio Committee on Health praised the ‘rapid response’ and ‘teamwork and effective management’ that prevented a far worse domestic situation. The Eastern Cape Department of Health was forced this week to debunk a fake social media notice claiming a hantavirus outbreak at Grey Hospital – a reminder that in the information environment of 2026, rumour and fear move faster than any pathogen.
WHAT AFRICA NEEDS TO KNOW
The Science of Reassurance: What Is True, What Is Uncertain, What Remains Unknown
The reassurances offered by both Harare and Johannesburg are grounded in epidemiological reality – but they are not without caveats that demand honest accounting.
The WHO’s assessment that the global risk from this event is low rests on two pillars. First, Andes virus human-to-human transmission, while documented, is rare and typically requires close, sustained contact with a symptomatic person – the kind of prolonged intimacy found between spouses or household members, not casual travellers. Second, the exposure chain in this outbreak traces clearly to the expedition cruise ship environment and specific ecological sites. There is no evidence of community spread in any country.
What the science also tells us, however, is that the incubation window is long – up to 42 days – that symptoms in their early phase are easily mistaken for influenza or COVID-19, and that when Hantavirus Pulmonary Syndrome progresses to its cardiopulmonary phase, it can kill within hours. The case fatality rate for HPS runs between 30 and 50 percent globally; this cluster has already exceeded that average. There is no licensed antiviral. There is no vaccine. Treatment is supportive care in an ICU – equipment and expertise are distributed unevenly across Africa.
Africa CDC has stated clearly that it is closely monitoring the situation, coordinating with the NICD and regional health authorities. The organisation notes that while hantavirus infections are rarely reported on the African continent, rodent reservoirs do exist, and surveillance is limited – meaning human cases are “likely being under-recognised.” This is a sentence that deserves to be read slowly.
For Zimbabwe, the specific concern is not that Andes virus will establish itself in the country – the long-tailed pygmy rice rat of South America is not a southern African resident – but that the healthcare workers under observation must be monitored with consistency and rigour for the full 45 days, regardless of how well they appear. Early symptoms are deceptively mild. The window between ‘feeling fine’ and ‘acute respiratory distress syndrome’ can be measured in hours.
The public health message from both governments is calibrated: proportionate alarm without panic; transparent disclosure without sensationalism; science-led action without the paralysis of uncertainty. It is the kind of response that public health requires and that African health systems — chronically underfunded, perpetually crisis-tested — have too rarely been positioned to deliver with full institutional credibility.
That both Harare and Johannesburg are managing to deliver it, in May 2026, is worth noting. Whether they can sustain it for 45 more days is the question that matters.
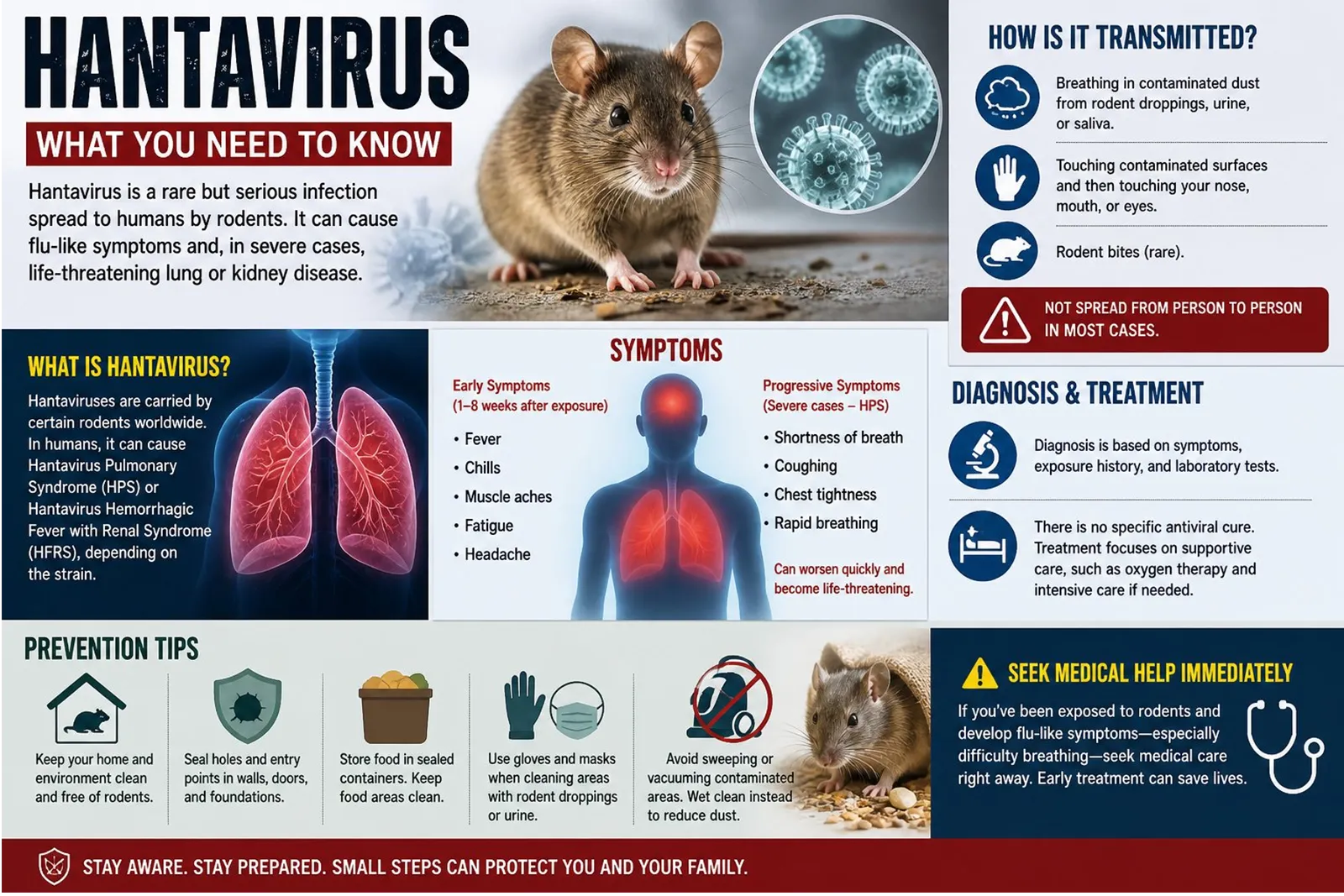
BACKGROUND: WHAT IS HANTAVIRUS? KEY FACTS FOR AFRICAN READERS
| HANTAVIRUS: WHAT YOU NEED TO KNOW ■ Hantaviruses are a family of 38+ known viruses carried by rodents. They do not typically make the rodent sick, but can cause severe, potentially fatal illness in humans. ■ Most hantaviruses infect humans through contact with infected rodent droppings, urine, or saliva — typically via inhaled aerosol. The Andes virus is the sole exception: the ONLY strain documented to transmit between humans, and only in cases of close, prolonged contact. ■ In the Americas, hantavirus causes Hantavirus Pulmonary Syndrome (HPS) — characterised by fever and gastrointestinal symptoms, rapidly progressing to pneumonia, acute respiratory distress syndrome, and shock. Case fatality rate: 30–50 percent. ■ Incubation: 4–42 days. Early symptoms — fever, fatigue, muscle ache, nausea — are easily confused with influenza or COVID-19. The cardiopulmonary phase can kill within hours of onset. ■ No licensed antiviral treatment or vaccine exists. Management is intensive supportive care: hospitalisation, oxygen, mechanical ventilation, ICU monitoring. Early care significantly improves survival. ■ The Andes virus is endemic to southern South America — Argentina, Chile, Bolivia, Brazil, Paraguay. It is NOT endemic to Africa. Africa has its own hantavirus strains (Sangassou, Tanganya, Azagny) in indigenous rodents, but surveillance is considered insufficient, and human cases are likely under-recognised. ■ WHO advises: anyone with a possible exposure history who develops fever, muscle ache, or respiratory symptoms within 42 days should seek immediate medical attention and disclose their contact history to clinicians. Sources: WHO DON599 (4 May 2026); Africa CDC (4 May 2026); US CDC HAN Advisory (May 2026); NICD South Africa Fact Sheet (May 2026). |